CELL
2000年,Cell期刊发表了由Robert Weinberg与Douglas Hanahan合著的《Hallmarks of Cancer》,这一里程碑式的概念框架深刻影响了癌症研究领域。值此发表25周年之际,Cell推出此次特刊,汇集了多篇综述、观点与评论文章,全面回顾与展望癌症研究框架的演进。
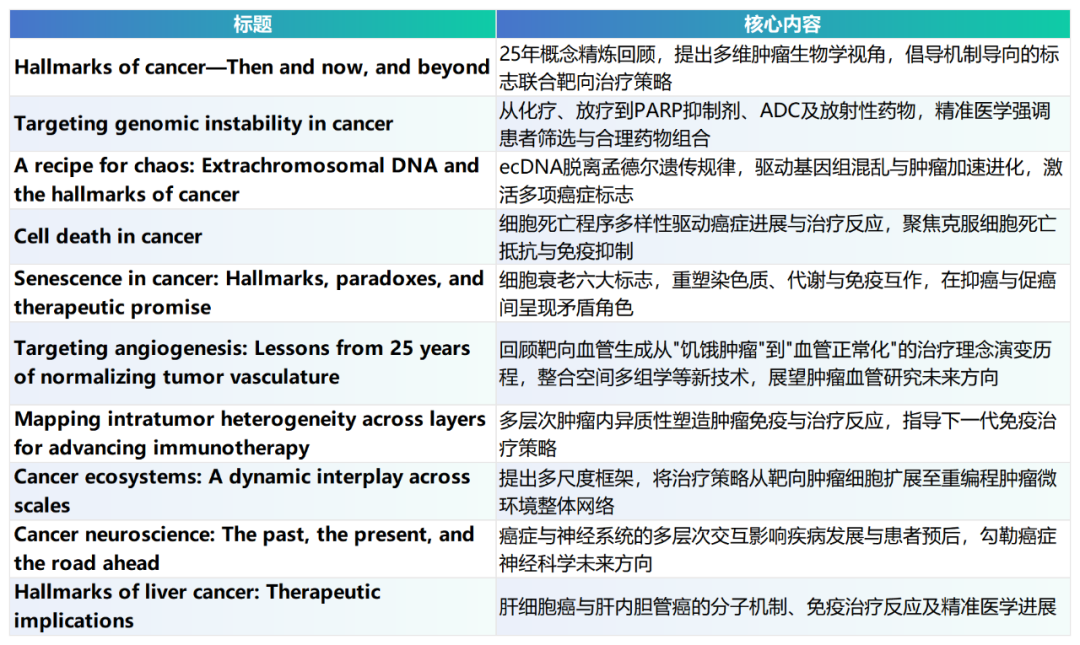
本期主要为10篇核心综述文章:
一、癌症标志:25年演进与多维框架的系统整合
Hallmarks of cancer—Then and now, and beyond
原文:https://www.cell.com/cell/fulltext/S0092-8674(25)01498-9
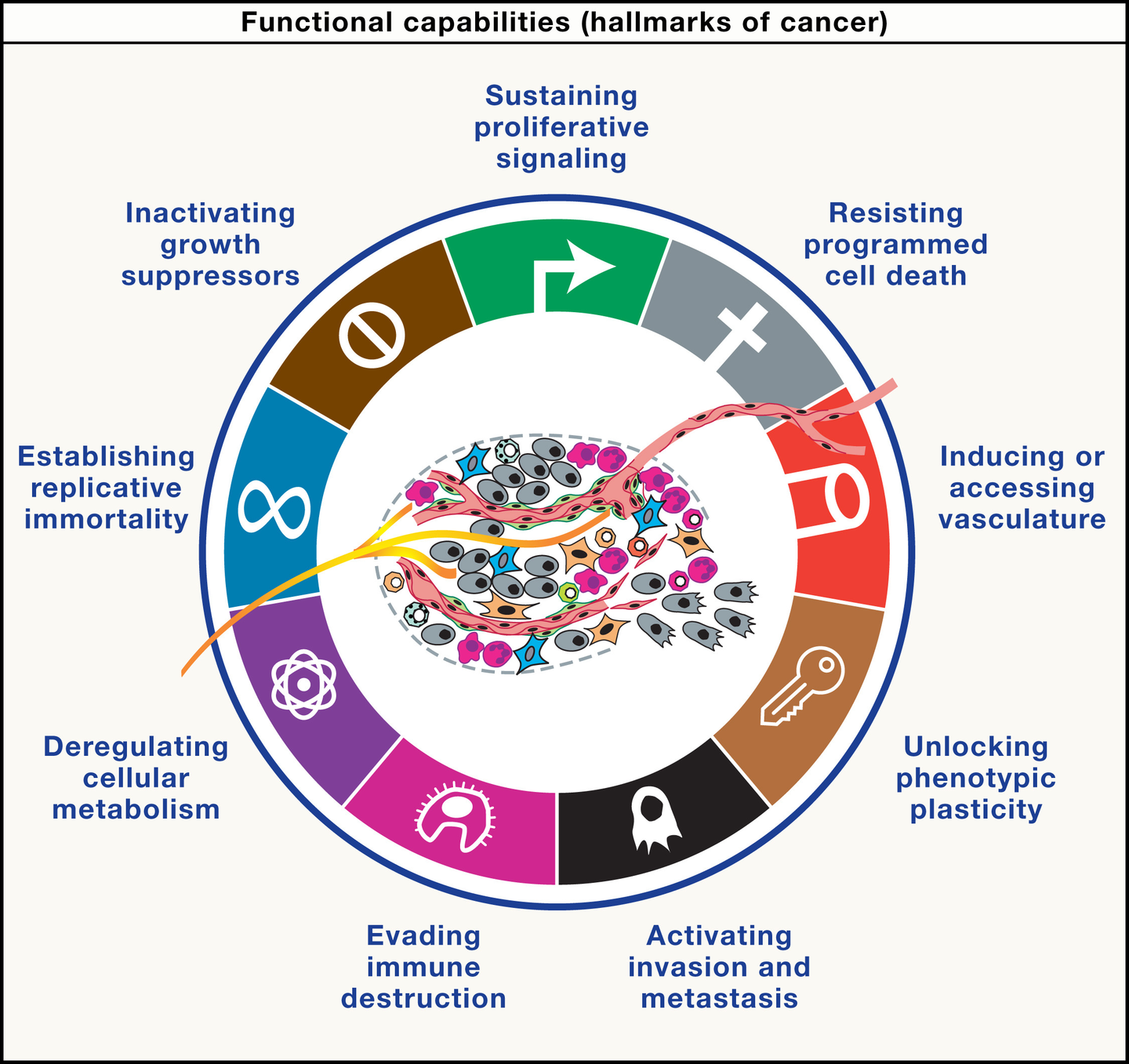
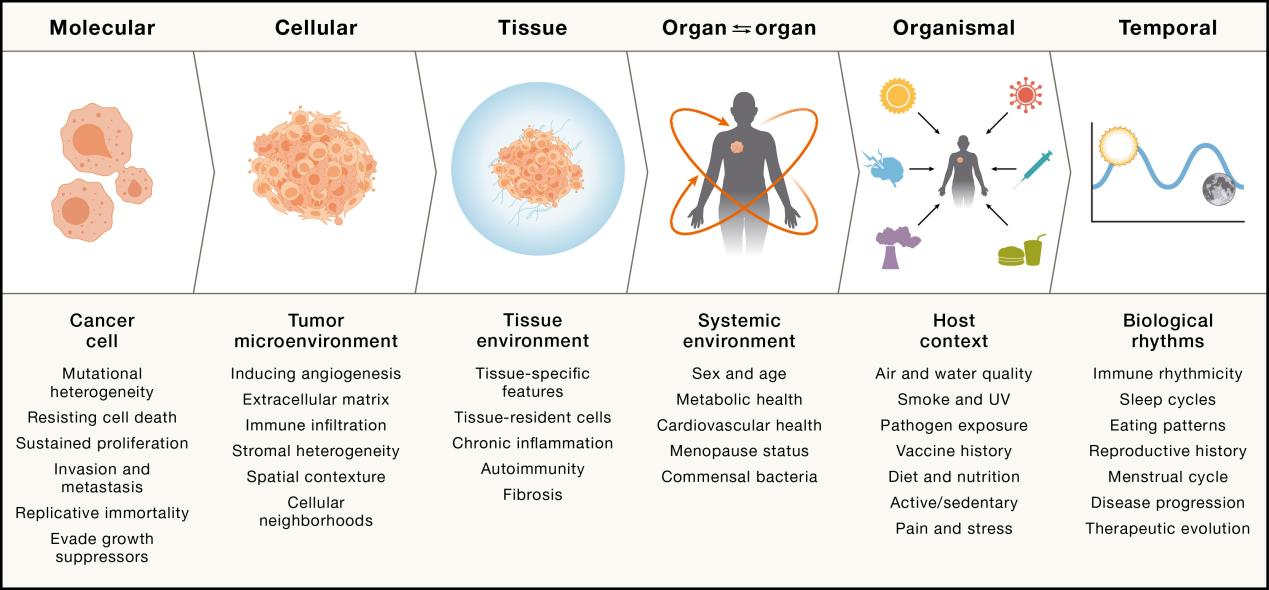
《癌症标志》框架自2000年提出至今已历经25年演进,从最初的六大功能特征扩展为一个涵盖四个维度的多层次体系:9项获得性功能能力(包括持续增殖、逃避免疫、侵袭转移等)、5项表型使能特征(如基因组不稳定性、表观遗传重编程、肿瘤神经支配等)、肿瘤微环境中的多类细胞组分(成纤维细胞、髓系细胞、神经元等),以及系统性宿主互作(衰老、肥胖、环境因素)。在治疗层面,该框架催生了"标志协同靶向"策略,通过同时阻断多个独立标志来克服适应性耐药,代表性组合包括抗血管生成联合免疫检查点抑制剂、PARP抑制剂联合抗VEGF等。结合单细胞测序与空间转录组学的进步,癌症标志框架正为精准肿瘤学提供愈加清晰的"操作系统"路线图。
Summary
Cancer presents a remarkably instructive perturbation of mechanisms manifesting in our biology that have gone awry, eliciting a malady that is inexorably increasing in incidence and societal burden concomitant with healthier aging. The wealth of knowledge and data forthcoming from decades of cancer research can be organized into conceptually distinct but interconnected parametric dimensions that define the mechanistic foundation of the disease: aberrantly acquired functional capabilities (the hallmarks of cancer), enabling phenotypic characteristics, hallmark-conveying cells populating cancer microenvironments, and systemic interactions. Collectively, they provide a logical framework with which to illuminate the operating systems of these outlaw organs, from inception through multistage tumorigenesis to adaptive evolution. This review presents a concise synthesis of the hallmark conceptualization as it has been refined during the past 25 years, including a corollary hypothesis that mechanism-guided hallmark co-targeting could offer impactful new therapeutic strategies for treating human cancers.
二、靶向基因组不稳定性:从合成致死到精准多维治疗的演进
Targeting genomic instability in cancer
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00336-3
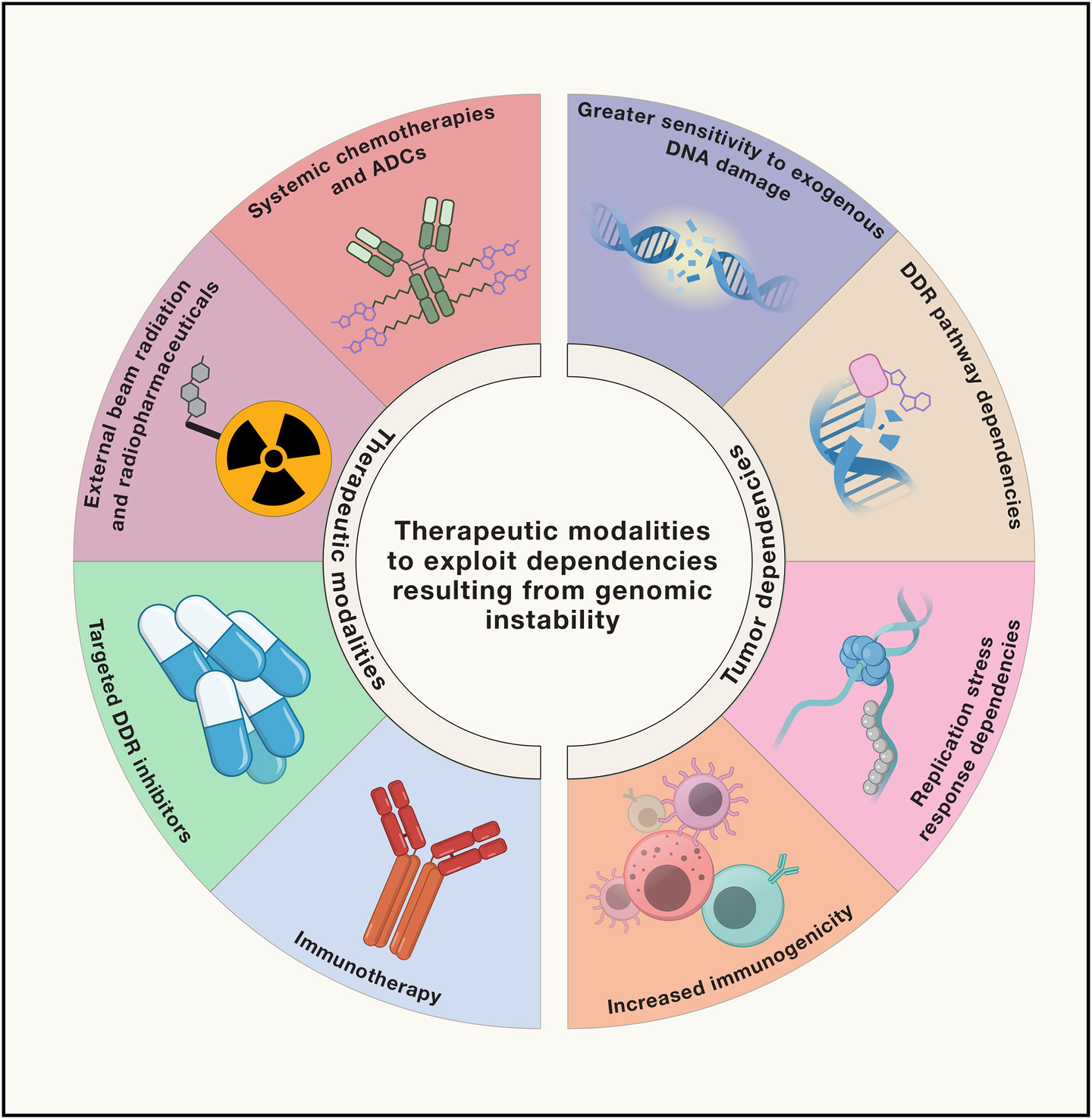
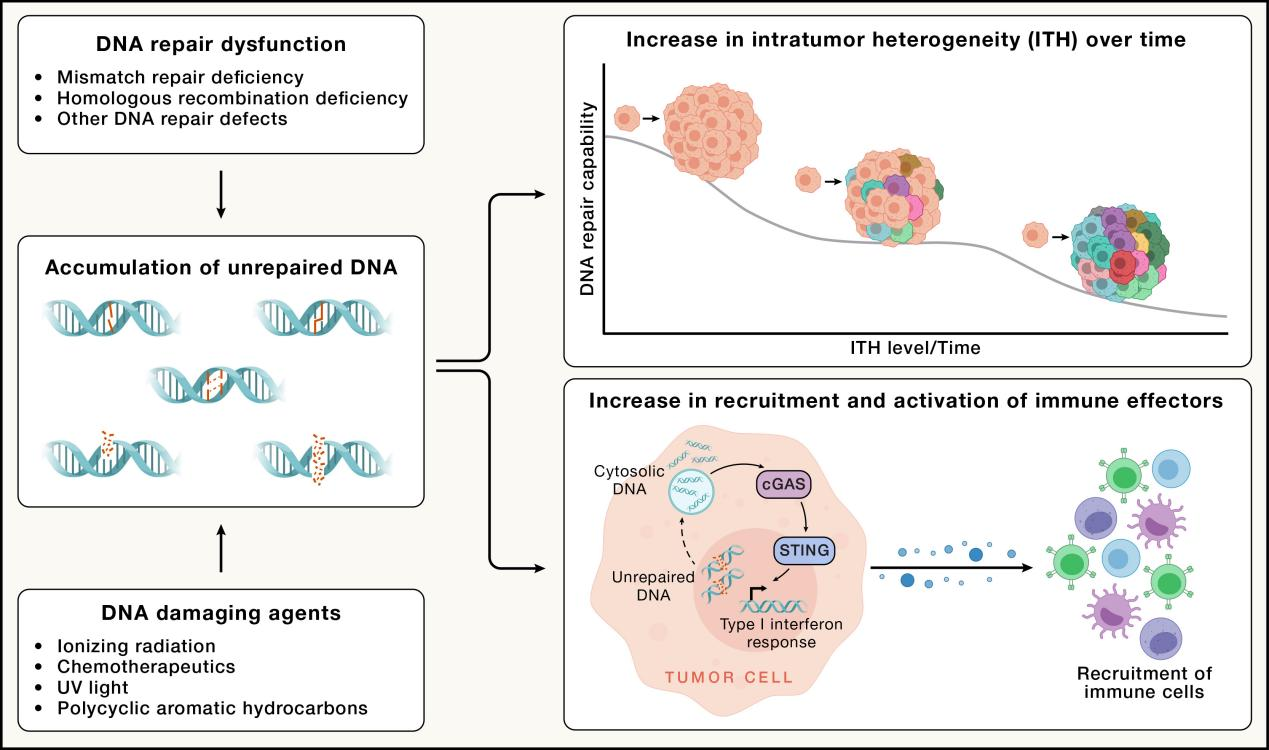
基因组不稳定性既是癌症恶性进化的核心驱动力,也是精准治疗的关键靶点。本综述系统梳理了靶向这一标志的治疗策略全貌:从20世纪40年代氮芥、铂类等经验性地毒性化疗的起源,到以PARP抑制剂(奥拉帕利等)为代表的合成致死精准疗法的临床验证,再延伸至新一代PARP1选择性抑制剂、ATR/CHK1/WEE1/PKMYT1等DDR通路靶向药物的系统布局。在肿瘤靶向递送层面,ADC通过将卡奇霉素、TOP1抑制剂、微管毒素等高效载荷精准输送至肿瘤细胞,显著拓宽了治疗窗口;放射性药物则借助β、α及俄歇电子等不同射线特性实现差异化DNA损伤。文章还深入阐释了基因组不稳定性与免疫系统的交互机制——通过cGAS-STING通路激活I型干扰素应答,为DDR抑制剂联合免疫检查点抑制剂提供了坚实的理论与临床依据(DUO-E试验)。此外,针对染色体不稳定性(CIN)、染色体外DNA(ecDNA)及TP53 Y220C突变的新兴靶向策略进一步拓展了治疗边界。未来方向聚焦于功能性HRD生物标志物开发、"间隔给药"策略优化及ADC与DDR抑制剂的协同组合,以推动癌细胞跨越"灾难性不稳定"阈值,同时最大限度保护正常组织。
Summary
Genomic instability is a defining feature of cancer, which arises when the cellular systems that maintain DNA integrity falter, enabling the accumulation of genetic and epigenetic alterations that drive malignant transformation. It is both the architect of cancer’s evolution and its Achilles’ heel. Targeting genomic instability has reshaped oncology: first through systemic chemotherapy and external beam radiation and then with poly(ADP-ribose) polymerase (PARP) inhibitors in homologous recombination repair-deficient tumors and other DNA damage response targets. Recently, tumor-targeted DNA-damaging platforms, namely antibody-drug conjugates (ADCs) and radiopharmaceuticals, have emerged alongside modern precision medicine strategies to optimize patient selection, develop rational combinations, and widen the therapeutic index.
三、染色体外DNA:打破孟德尔遗传规律的癌症混乱引擎
A recipe for chaos: Extrachromosomal DNA and the hallmarks of cancer
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00278-3
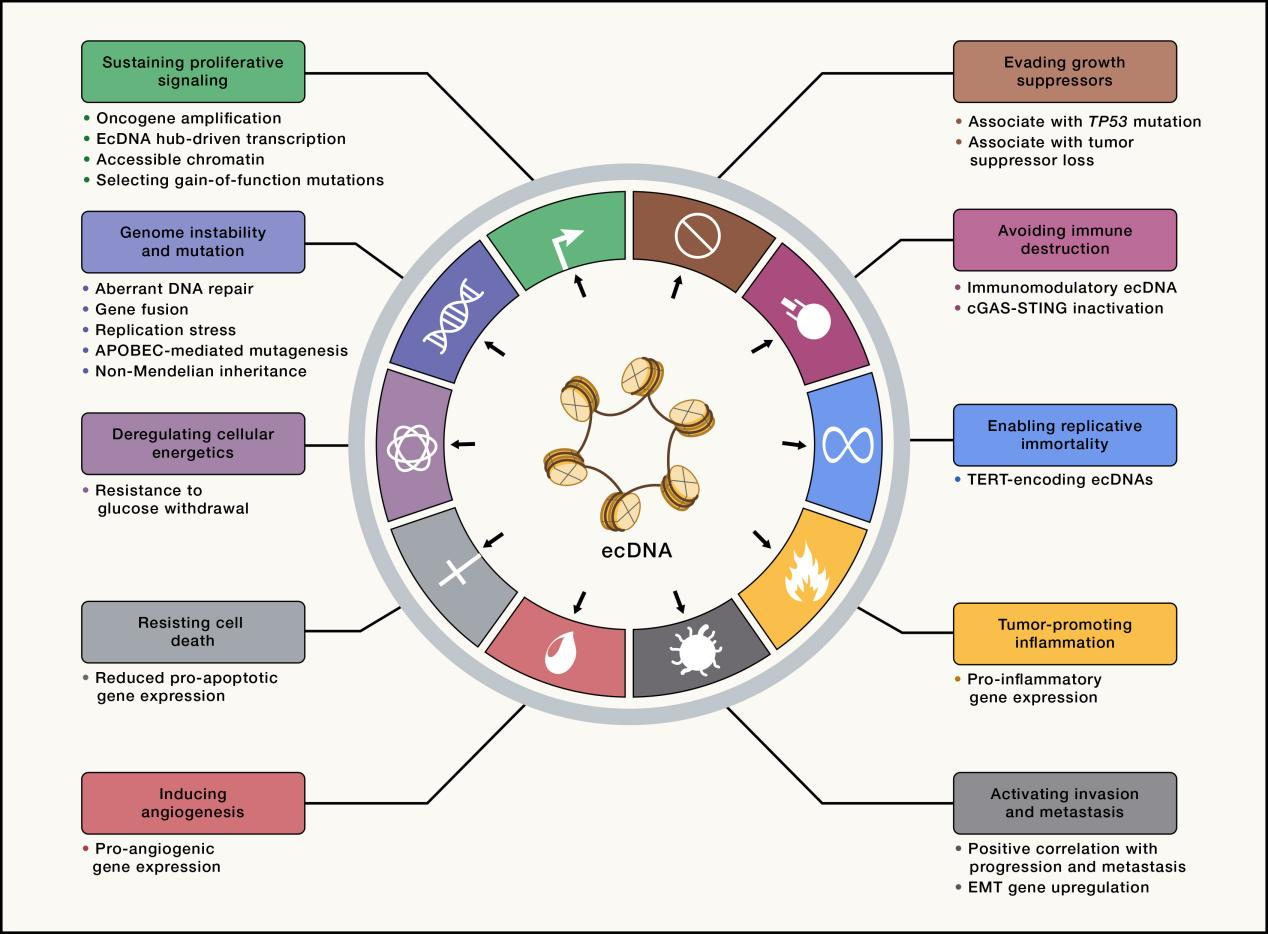
染色体外DNA(ecDNA)是一类缺乏着丝粒与端粒的兆碱基级环状DNA分子,存在于约17%的成人肿瘤和18%的儿童肿瘤中。由于早期测序分析默认将reads比对至参考基因组,ecDNA长期被忽视,直至2014年胶质母细胞瘤研究揭示其编码EGFRvIII,才引发范式转变。ecDNA通过增强子劫持和ecDNA核中心(Hub)的分子间协同转录,将MYC、EGFR、CDK4、TERT等癌基因推至全基因组表达量前1%;其非孟德尔随机分离特性导致极高的肿瘤内异质性,并通过有丝分裂"搭便车"机制确保自身传递,从而驱动癌症的快速克隆进化与耐药。在免疫层面,ecDNA阳性肿瘤系统性下调MHC I/II类分子,部分ecDNA甚至直接携带PD-L1(CD274)等免疫调控基因,同时沉默cGAS-STING通路以逃避胞质DNA监控,构建高度免疫抑制的肿瘤微环境。ecDNA与几乎所有癌症标志相关联,包括代谢重编程、复制永生化、侵袭转移及抵抗细胞死亡。治疗层面,靶向ecDNA Hub的BET抑制剂、利用转录-复制冲突的复制应激策略及基于液体活检片段组学的诊断工具正在积极开发中,有望将ecDNA这一肿瘤进化的"混乱引擎"转化为精准治疗的新靶点。
Summary
Some aggressive cancers exhibit a level of rapid genome change and therapy resistance that is difficult to explain. Research over the past decade has shown that extrachromosomal DNA (ecDNA) can be the cause. When oncogenic genetic elements untether from chromosomes and no longer follow Mendelian inheritance, genomic chaos and accelerated evolution ensue, generating unique ecDNA biology and non-traditional therapeutic vulnerabilities distinct from traditional mutation-targeting approaches. Here, we put forward a holistic view where ecDNA is integrated into the broader Hallmarks of Cancer framework to better understand the problem and chart a path forward.
四、癌症中的细胞死亡逃逸与重激活:从分子机制到临床转化的系统性综述
Cell death in cancer
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00325-9
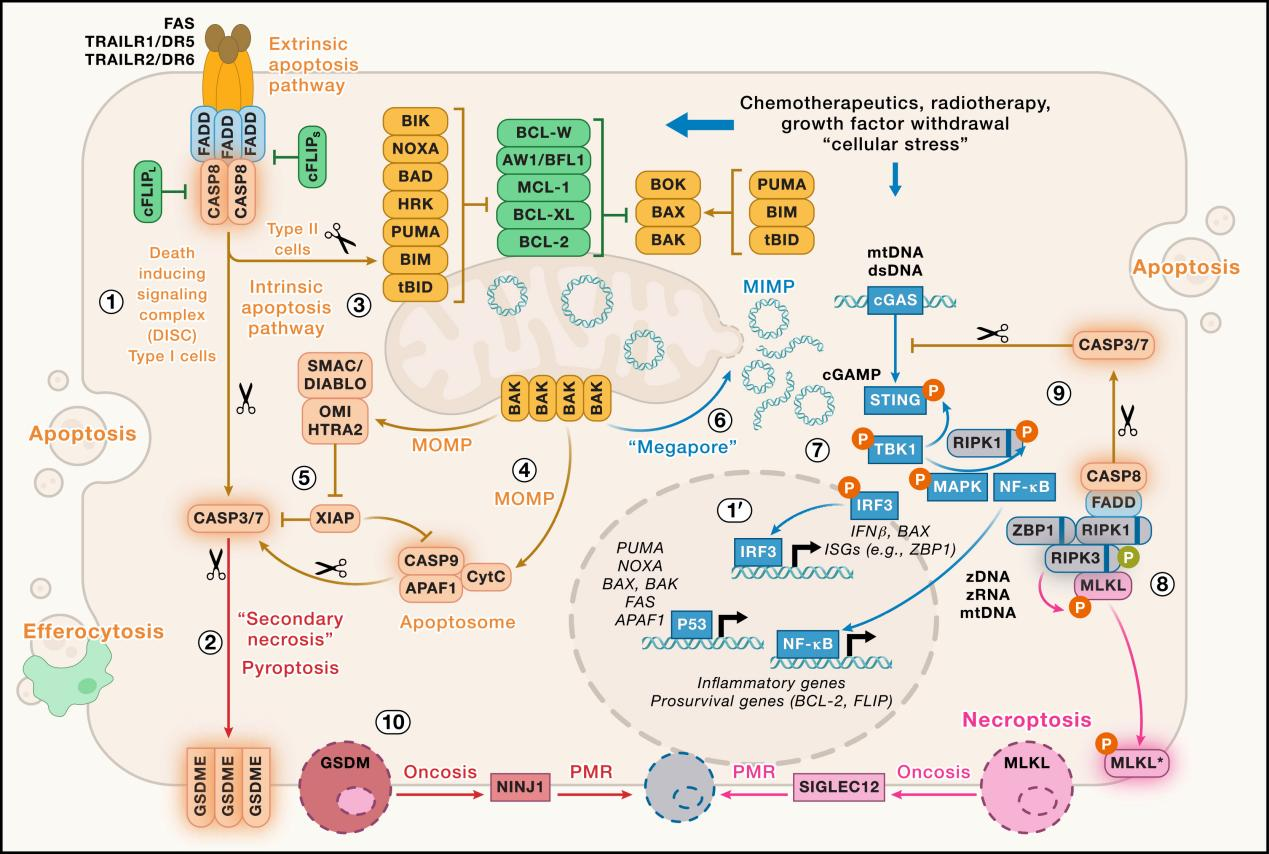
全面梳理了癌症中调节性细胞死亡(RCD)的多种模式及其治疗潜力。癌细胞通过多种机制逃避死亡程序,是肿瘤进展与治疗耐药的核心驱动力。文章重点阐述了五大死亡通路:①凋亡——BCL-2家族调控线粒体通透性,Venetoclax等BH3模拟物已在CLL/AML中取得突破性临床成效;②坏死性凋亡——RIPK1/RIPK3/MLKL信号轴介导的炎性裂解性死亡,癌细胞常通过RIPK3启动子甲基化实现逃逸;③焦亡——Gasdermin家族蛋白打孔执行,可将"冷"肿瘤转化为免疫"热"肿瘤,但也可能诱发细胞因子释放综合征;④铁死亡——GPX4/FSP1轴调控脂质过氧化,药物耐受持留细胞(DTP)对GPX4高度依赖,是克服耐药的潜在靶点;⑤铜死亡、二硫键死亡等新兴代谢性死亡模式,拓展了肿瘤代谢脆弱性的治疗边界。在免疫层面,免疫原性细胞死亡(ICD)通过释放DAMPs激活抗肿瘤免疫,NINJ1作为质膜破裂的通用介质发挥关键放大作用。临床转化面临生物标志物缺乏、系统毒性及实体瘤复杂性等挑战(如VERONICA、TrilynX试验的失败)。未来方向在于理性联合用药——将RCD诱导剂与免疫检查点阻断(ICB)、代谢调节剂协同整合,实现个体化精准杀伤耐药肿瘤克隆。
Summary
“Evasion of cell death” is a hallmark of cancer, enabling transformed cells to withstand oncogenic and therapeutic stress. Restoring cancer cell death is an appealing strategy but requires a deep understanding of cell death programs. Over the past two decades, the cell death field has expanded from apoptosis to include necroptosis, pyroptosis, ferroptosis, and other emerging programs, reshaping cancer biology and revealing therapeutic opportunities. While apoptosis remains the primary radiation- and chemotherapy-induced cell death program, non-apoptotic programs can drive inflammatory responses and orchestrate the interplay among tumor, stroma, and immune components, influencing immunotherapy outcomes. Ferroptosis, an iron-dependent, lipid peroxidation-driven cell death modality, lacks a canonical induction signal and arises from perturbations in lipid, iron, and redox metabolism. This review presents a unified framework for understanding the roles of major cell death programs in cancer development, progression, and treatment response, as well as addressing resistance to cancer cell death and immune suppression.
“Our bodies are made of cells that live, and just as surely, of cells that must die.” –S. Brenner
五、细胞衰老在癌症中的双重角色:从分子机制、悖论特征到靶向治疗
Senescence in cancer: Hallmarks, paradoxes, and therapeutic promise
原文:https://www.cell.com/cell/abstract/S0092-8674(26)00272-2
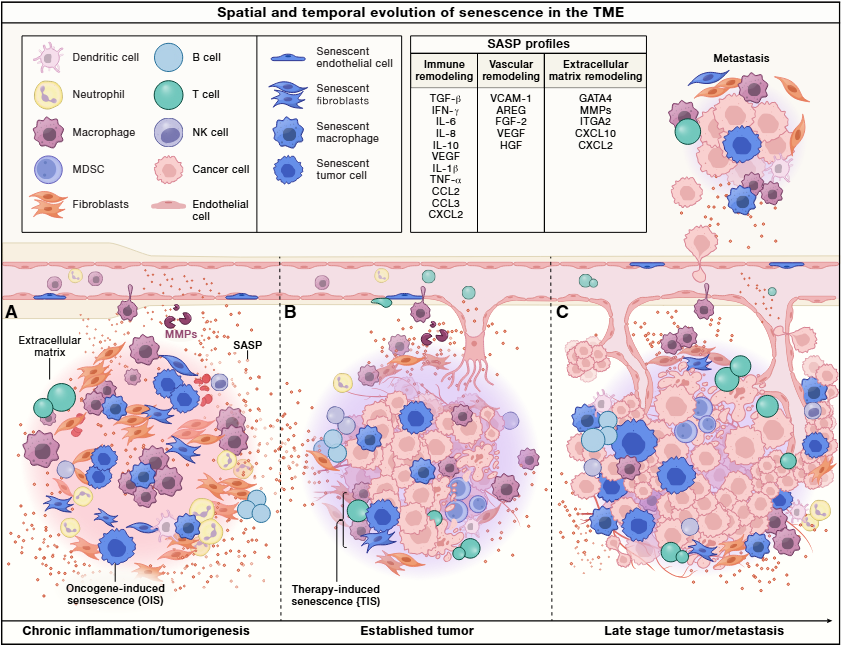
细胞衰老自1961年Hayflick发现以来,已从体外现象演变为肿瘤抑制与促进的"双刃剑"程序。文章提出衰老的六大标志性维度:稳定的增殖阻滞(p53/p21与p16/RB通路)、染色质与核结构重塑(SAHFs形成、Lamin B1丢失)、抗细胞死亡能力增强(BCL-2/BCL-XL/BCL-W上调)、衰老相关分泌表型(SASP)(IL-6、MMP等炎性因子大量分泌)、微环境感知重编程(uPAR、NK细胞配体等表面蛋白重塑)以及代谢异常激活(ROS升高、溶酶体扩张)。在肿瘤抑制层面,癌基因诱导衰老(OIS)是细胞对KRAS/BRAF等强烈致癌信号的"熔断"响应,免疫系统通过NK细胞、CD8⁺ T细胞等实施衰老监控以清除衰老细胞;而一旦监控失效,持续存在的衰老癌相关成纤维细胞(CAFs)则通过SASP重塑免疫抑制微环境,反向促进肿瘤进展,体现出拮抗多效性的核心悖论。治疗策略上,文章提出三大方向:①Senolytics(靶向清除衰老细胞),包括Navitoclax、D+Q组合及uPAR靶向CAR-T细胞;②Senomorphics(抑制SASP),涵盖JAK抑制剂、BET抑制剂及雷帕霉素;③**"两步拳"策略**——先以CDK4/6抑制剂或低剂量化疗诱导治疗性衰老(TIS),再联合Senolytic或PD-1/PD-L1免疫检查点阻断清除衰老肿瘤细胞。未来挑战在于体内衰老生物标志物匮乏、衰老表型高度异质性("Senotypes")以及靶向治疗的系统毒性,精准干预病理性衰老、同时保护其生理功能,将是癌症与衰老相关疾病治疗的重要突破方向。
Summary
Cellular senescence is a conserved stress-responsive program defined by durable proliferative arrest and extensive remodeling of chromatin, metabolism, intercellular signaling, and immune interactions. Initially described as a barrier to unlimited cell division, senescence is now recognized as a pleiotropic and heterogeneous biological process with roles in development, tissue repair, immune surveillance, tumor suppression, aging, fibrosis, and cancer progression. Despite its broad relevance, senescence remains challenging to define operationally, as its molecular features, functional outputs, and physiological consequences vary across cell types, tissues, and stimuli. This review summarizes core hallmarks of senescence while synthesizing how these features are differentially engaged, diversified, and repurposed across biological contexts. Focusing on cancer, we discuss how senescence influences tumor initiation, evolution, and therapeutic response through both cell-intrinsic and microenvironmental mechanisms. We further evaluate emerging strategies to therapeutically modulate senescence, highlighting both opportunities and unresolved challenges for precision intervention.
六、肿瘤血管正常化理论的演进与临床转化:抗血管生成治疗25年的经验与启示
Targeting angiogenesis: Lessons from 25 years of normalizing tumor vasculature
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00283-7
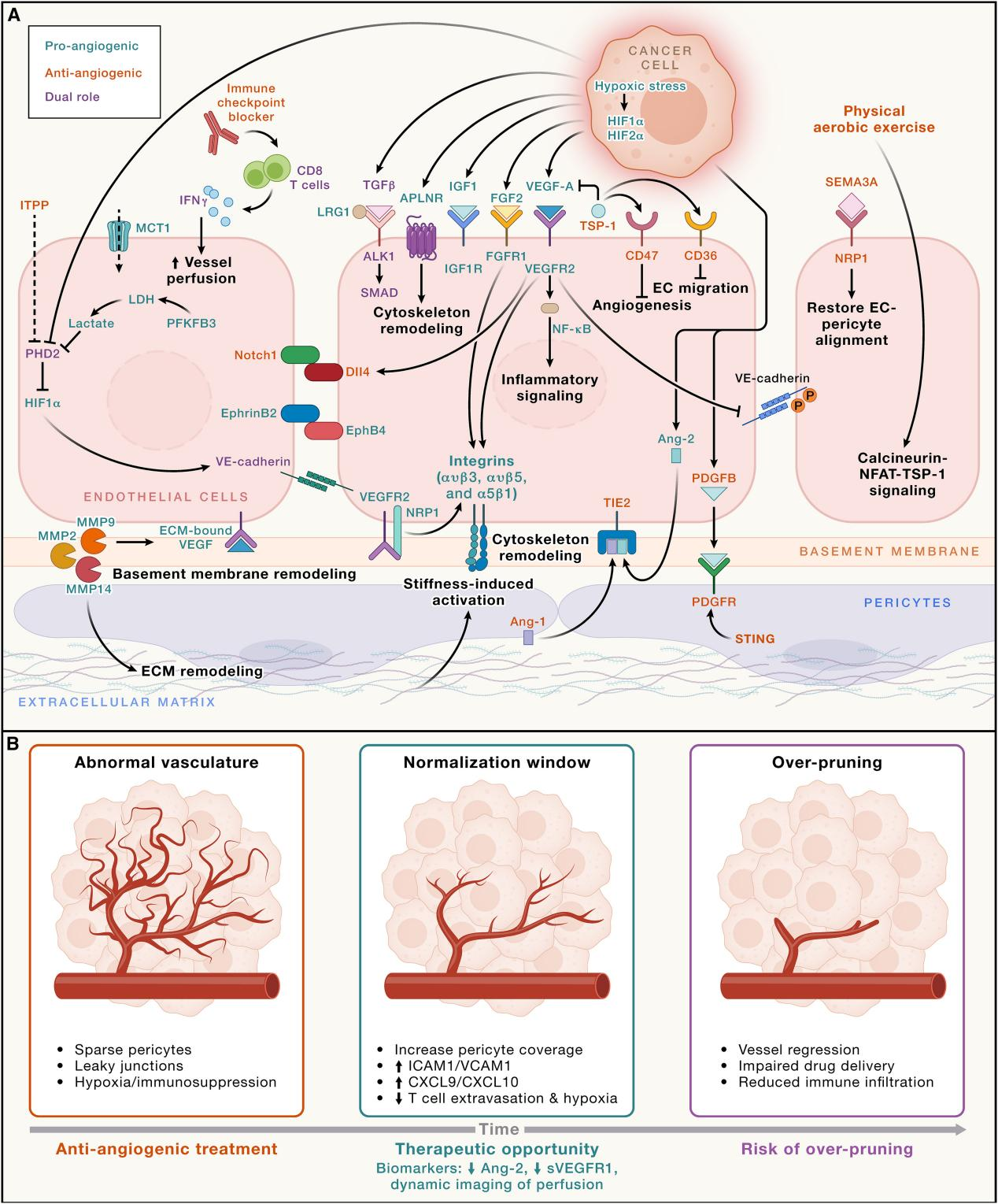
肿瘤的生长与转移高度依赖异常血管网络的形成。自1971年Folkman提出肿瘤生长依赖血管生成的里程碑假说以来,该领域历经25年发展,于2001年由Jain提出颠覆性的血管正常化假说——即通过适度抑制而非彻底摧毁肿瘤血管,修复其结构与功能,从而改善药物递送与治疗效果。肿瘤血管的核心病理特征包括:高度迂曲、基底膜不完整、周细胞覆盖不足及高通透性,导致组织间液压升高、缺氧与酸性微环境形成,进而激活HIF1α-VEGF正反馈回路,持续驱动无效血管生成。在分子机制层面,VEGF-VEGFR2轴、Ang2介导的血管失稳、Notch-DLL4调控的尖端/茎细胞比例失衡是关键靶点。更重要的是,异常血管通过抑制黏附分子表达、上调FasL等机制构成免疫屏障,阻碍T细胞浸润。临床实践已证实,抗VEGF联合免疫检查点抑制剂(如阿替利珠单抗+贝伐珠单抗用于HCC,仑伐替尼+帕博利珠单抗用于RCC)是当前一线标准方案。未来方向聚焦于双特异性抗体(如Ivonescimab)、纳米递药系统及武装型CAR-T细胞等新一代平台,同时亟需开发精准生物标志物以识别个体化的"血管正常化窗口期",推动肿瘤血管重编程走向真正的精准治疗。
Summary
Tumors acquire blood vessels primarily via sprouting angiogenesis and co-option of pre-existing host vasculature, but also via intussusception, vasculogenesis from bone-marrow-derived progenitors, vascular mimicry, and endothelial transdifferentiation. The abnormal structure and function of these vessels, resulting from an imbalance between pro- and anti-angiogenic signaling as well as from the physical forces, impair the delivery and efficacy of therapeutics. We review the evolving narrative of targeting angiogenesis from starving tumors to vascular normalization as a therapeutic principle and highlight recent spatial-omics revelations and the emerging role of neural, microbial, hormonal, and chronological factors. We elaborate on the molecular mechanisms of tumor vessel formation, how dysfunctional vessels cause an abnormal tumor microenvironment characterized by hypoxia, low pH, elevated fluid pressure, and immunosuppression, and how vascular normalization enhances the delivery and efficacy of various therapies, including immunotherapies, and has formed the basis of emerging strategies and novel therapeutic agents to improve patient outcomes.
七、肿瘤内异质性的多维图谱解析:推动免疫治疗精准化的理论框架与策略展望
Mapping intratumor heterogeneity across layers for advancing immunotherapy
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00326-0
肿瘤内异质性(ITH)是涵盖基因组、表观遗传、转录、蛋白质及免疫肽组多个层次的复杂现象,是肿瘤免疫逃逸与治疗耐药的核心驱动力。在遗传层面,克隆性新抗原比亚克隆性新抗原能诱导更强的免疫应答,而错配修复缺陷(MMRd)、染色体不稳定性(CIN)及染色体外DNA(ecDNA)等基因组不稳定机制则持续扩大肿瘤异质性;在非遗传层面,细胞状态的可塑性转换(如EMT、药物耐受持留细胞DTP)使肿瘤在无新突变的情况下实现快速适应。免疫肽组作为细胞内部状态的"表面读出",其异质性由顺式(肽序列突变)与反式(RNA剪接、翻译保真度、蛋白酶体加工)因素共同决定,直接影响T细胞识别效率。在抗原靶向策略上,研究者正从简单的TMB预测转向持久性TMB(pTMB)、驱动突变来源新抗原(如RAS.Q61K)及非基因组编码抗原等更稳定的靶点。此外,以NeoPrecis为代表的AI模型整合新抗原免疫原性与肿瘤进化信息,预测免疫检查点抑制剂(ICB)疗效的AUC提升达11%–20%。未来的治疗策略需围绕"扩大抗原覆盖、稳定MHC-I呈递、重塑免疫微环境、促进旁观者杀伤"四个维度协同推进,从描述异质性走向预判并前置干预肿瘤进化逃逸,实现真正意义上的精准免疫治疗。
Summary
Intratumor heterogeneity (ITH) encompasses genetic, epigenetic, transcriptional, proteomic, and immunopeptidomic diversity. Beyond genetic heterogeneity, it is increasingly clear that non-mutational heterogeneity and plasticity generate dynamic cancer cell states with distinct immune visibility. These layers of complexity converge on the immunopeptidome, the repertoire of peptides displayed by major histocompatibility complex molecules through which tumor cells are surveyed by T cells. Variation in antigen processing, presentation, and peptide abundance across cancer clones and cell states yields spatially and temporally distinct immunological niches that shape immune recognition and therapeutic response. Here, we summarize how multidimensional ITH manifests across cancer types and constrains immunotherapy efficacy. We propose that integrating measurements across layers is a promising direction for improving biomarker identification and informing more precise immune-based treatment strategies.
八、肿瘤生态系统的跨尺度动态整合:从微环境重塑到精准肿瘤学的系统性框架
Cancer ecosystems: A dynamic interplay across scales
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00270-9
TME已从"局部背景"演变为决定肿瘤进展与治疗结局的核心生态系统。本文提出一个跨分子、细胞、组织、机体及环境五个尺度的整合性框架。在结构层面,癌症相关成纤维细胞(CAFs)通过构建异质性ECM物理屏障限制T细胞浸润,转录组解析超万例肿瘤后识别出免疫炎症型、免疫排斥型、免疫低下型和中性粒细胞富集型四种泛癌微环境亚型;在时间维度上,TME随免疫压力与治疗干预持续演化,**TCF1+祖先耗竭T细胞(pTEX)**及"免疫三联体"空间结构(CD8+ T细胞、CXCL13+ CD4+ T细胞、CCR7+ mregDC)是ICB应答的关键预测指标;在系统层面,性别(雄激素受体驱动T细胞耗竭)、衰老(IL-1α介导的紧急髓系造血)、肥胖悖论、PM2.5促癌等宿主生理因素深刻调控抗肿瘤免疫;此外,肠道菌群(FMT可将ICB客观缓解率提升至65%)、昼夜节律(CAR-T与ICB疗效具有时相依赖性)、运动(激活NK细胞并增强T细胞线粒体功能)等可干预因素正成为新兴治疗轴。未来精准肿瘤学须融合空间组学精准定位、纵向动态采样、AI多维整合分析与生理条件调控,实现从短暂控瘤到持久治愈的根本性跨越。
Summary
Tumors evolve within complex, adaptive ecosystems that operate across spatial, temporal, and systemic scales. Within each tumor microenvironment, numerous diverse cell populations assemble into specialized niches that are continually shaped by systemic physiology, environmental inputs, and therapeutic pressure. Beyond the local microenvironment, cancer progression is governed by the host macroenvironment, where intrinsic biological determinants intersect with modifiable factors to collectively impact physiological fitness and tissue resilience. Here, we propose a multi-scale framework that unites tumor biology with organismal physiology and reframes therapy from eliminating malignant cells in isolation to reprogramming the cellular, vascular, and systemic networks that sustain disease. We highlight emerging approaches that aim to restore physiological equilibrium, spanning from spatial multi-omics and AI-driven pathology to immune-vascular normalization and physiological conditioning. Together, these dimensions define an integrative vision for precision oncology that bridges discovery and intervention to achieve durable and ultimately curative cancer therapy.
九、肿瘤神经科学的机制解析与治疗转化:神经系统作为癌症调控核心轴的研究进展与前沿展望
Cancer neuroscience: The past, the present, and the road ahead
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00285-0
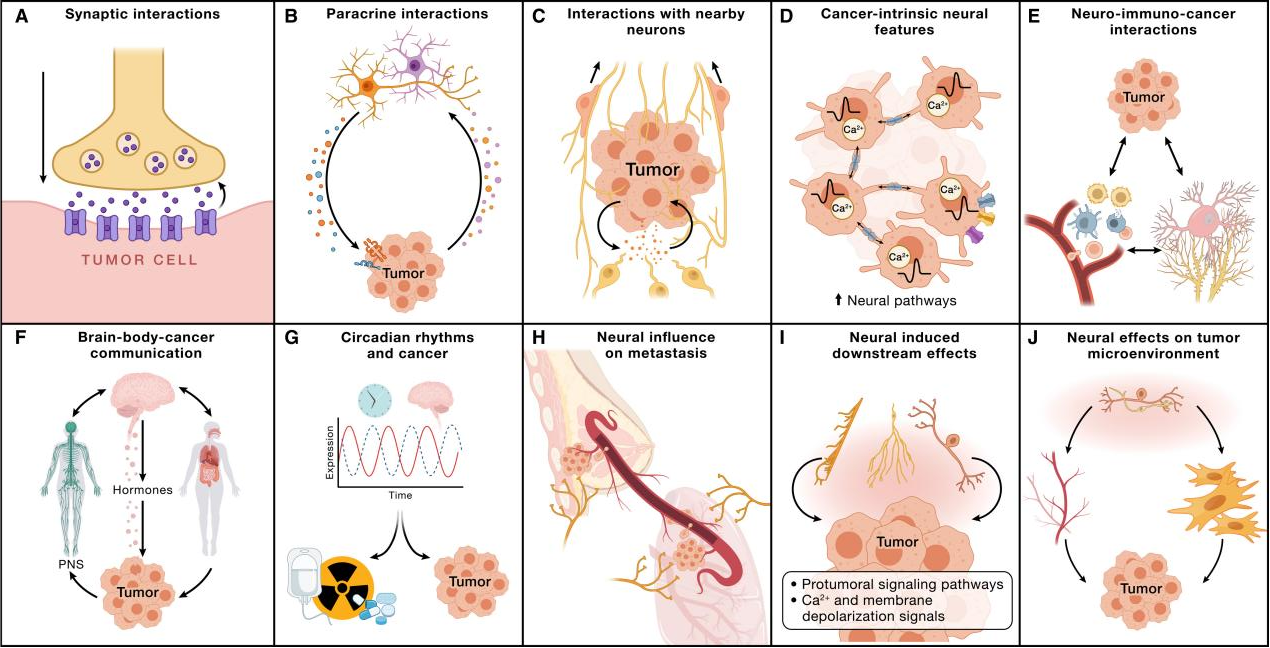
肿瘤神经科学作为新兴交叉领域,揭示了神经系统与肿瘤之间的双向调控关系,并将其确立为癌症的新兴核心标志之一。在直接神经调控层面,研究证实肿瘤细胞可与神经元形成功能性突触连接:胶质母细胞瘤通过激活Ca²⁺通透性AMPA受体(GluA2Q)接受谷氨酸能输入,弥漫性中线胶质瘤(DMG)则因高胞内氯离子浓度使GABA信号产生促增殖的去极化效应;在外周,交感神经(肾上腺素能)普遍促进肿瘤侵袭性,而副交感神经通常发挥抑制作用。在肿瘤内源性神经特征方面,胶质瘤细胞通过表达GAP-43、Ttyh1等神经发育驱动因子形成肿瘤微管(TMs)网络,借助缝隙连接传递Ca²⁺信号,赋予肿瘤对放化疗的高度抵抗性。在神经-免疫轴层面,伤害性感觉神经元释放的CGRP驱动CD8⁺ T细胞耗竭,β1-肾上腺素受体信号抑制T细胞增殖与细胞因子分泌,共同构筑免疫抑制微环境。在系统层面,大脑-机体-肿瘤轴通过HPA轴激活、昼夜节律紊乱(BMAL1/PER2缺失促进免疫逃逸)及睡眠期循环肿瘤细胞(CTCs)脱落峰值等机制深度影响肿瘤转移。在治疗转化方面,神经科学指导的肿瘤治疗(NiCT)已进入临床探索阶段,包括AMPA受体拮抗剂Perampanel(PerSurge II期试验)、β受体阻滞剂普萘洛尔联合免疫治疗,以及靶向神经发育程序等策略。未来十年的核心议题在于阐明泛癌神经机制、优化NiCT与现有疗法的协同方案,并探索迷走神经刺激等非药物干预手段,推动肿瘤治疗从细胞靶向迈向神经-免疫-肿瘤系统性整合的新范式。
Summary
Both the nervous system and cancer-intrinsic neural features can govern cancer initiation, growth, progression, metastasis, and treatment resistance, while cancer can likewise influence the nervous system, promoting neural reprogramming and neuropsychiatric symptoms that worsen patient outcomes. The field of cancer neuroscience seeks to unravel this complex neuro-cancer crosstalk and holds the promise to develop neuroscience-instructed cancer therapies that improve disease control and quality of life. Here, we summarize the key discoveries of neuro-cancer crosstalk to date, including neuron-to-cancer synapses and paracrine and neuro-immuno-oncological interactions, and then explore emerging topics such as downstream effects on cancer cell pathophysiology, circadian influences, brain-body-cancer communication, and neural regulation of the metastatic cascade and the tumor microenvironment. Finally, we distill overarching principles, highlight relevant ongoing research, and outline conclusions to guide the development of cancer neuroscience, proposing hypotheses for future experimental validation.
十、原发性肝癌的癌症标志解析与治疗转化:肝细胞癌与肝内胆管癌的分子病理、免疫治疗及精准肿瘤学进展
Hallmarks of liver cancer: Therapeutic implications
原文:https://www.cell.com/cell/fulltext/S0092-8674(26)00268-0
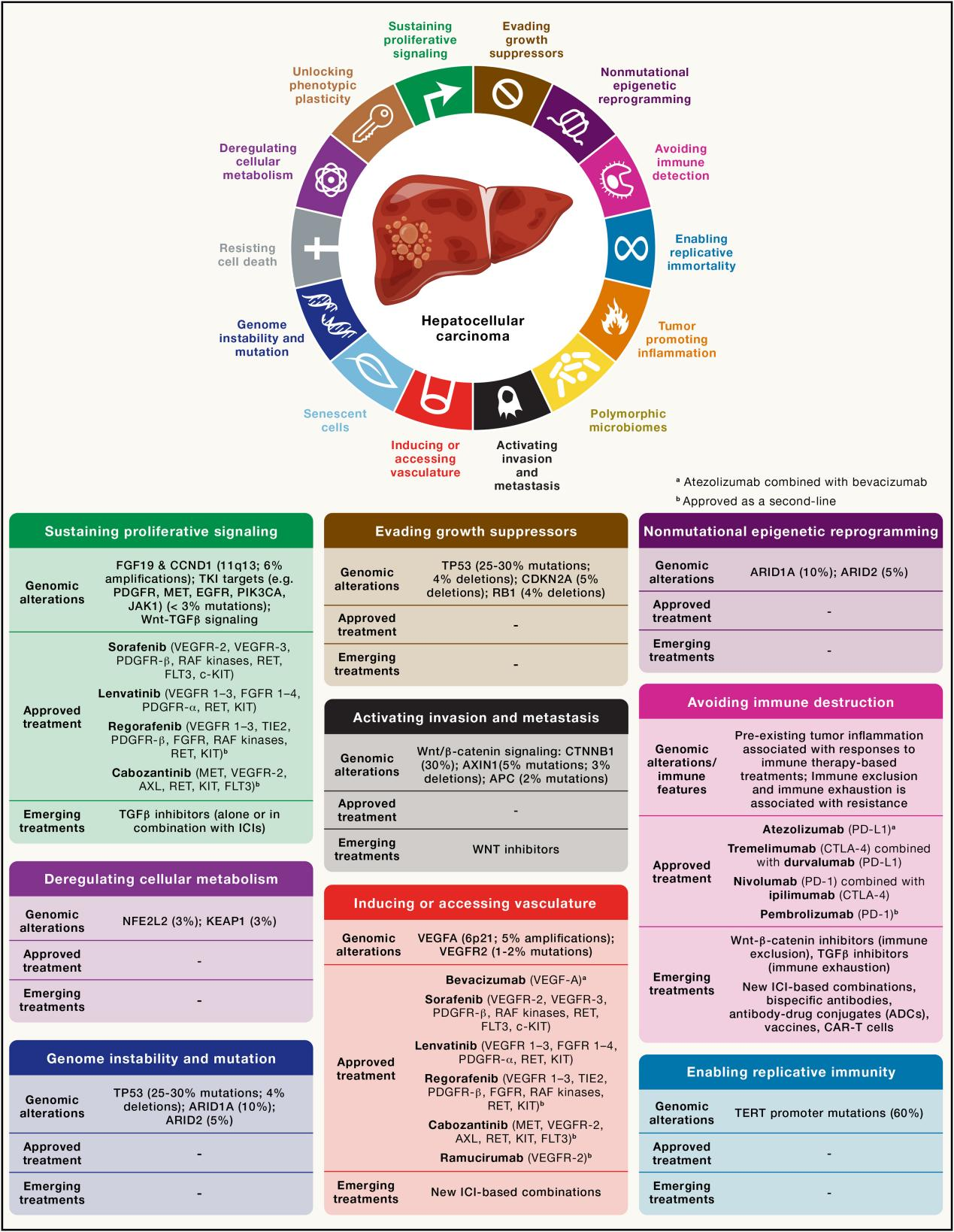
原发性肝癌是全球癌症相关死亡的第三大原因,预计至2050年年新发病例将达150万例,其中肝细胞癌(HCC)占85%–90%,肝内胆管癌(iCCA)占10%–15%。两者均呈现低肿瘤突变负荷与免疫抑制性微环境的共同特征,但在精准治疗可及性上差异显著。HCC基因组以TERT启动子突变(56%)、TP53突变(31%)及CTNNB1突变(25%)为主要驱动事件,仅约25%携带潜在可靶向突变;其高度血管依赖性使抗VEGF联合免疫检查点抑制剂(如阿替利珠单抗+贝伐珠单抗)成为当前一线标准方案,CheckMate 9DW研究中纳武利尤单抗+伊匹木单抗实现了36%的客观缓解率,为迄今晚期HCC最高应答率。iCCA则以高度纤维增生性间质和丰富的可靶向基因组改变为特征,约45%携带FGFR2融合、IDH1突变、BRAF V600E等驱动变异,Pemigatinib、Futibatinib及Ivosidenib等靶向药物已获批上市;一线方案吉西他滨+顺铂+Durvalumab(TOPAZ-1)将24个月生存率提升至约25%。在免疫逃逸机制上,HCC中CTNNB1突变亚型(20%)呈现典型"免疫沙漠"表型,对抗PD-1/PD-L1治疗天然耐药,是当前亟待攻克的难题。展望未来,AI放射组学(AUC达0.75–0.89)、GPC3靶向CAR-T细胞、GNOS-PV02个性化新抗原疫苗及微生物组干预等新兴策略正加速推进,有望将肝癌治疗从经验性用药全面迈向基于分子分型的精准免疫-靶向联合治疗新时代。
Summary
The hallmarks of cancer, first proposed in 2000, have since provided a unified framework for understanding the complexity of carcinogenesis. This conceptual model has profoundly influenced the treatment landscape of primary liver cancer, which includes hepatocellular carcinoma (HCC, ∼85%) and intrahepatic cholangiocarcinoma (iCCA, 10%)—malignancies with high mortality. Key hallmarks exhibited by HCC include sustaining proliferative signaling, inducing or accessing vasculature, and avoiding immune detection. Over the past two decades, outcomes for patients with advanced HCC have significantly improved with immunotherapies. iCCA is characterized by hallmarks such as sustaining proliferative signaling, deregulating cellular metabolism, and avoiding immune detection. Unlike HCC, roughly 45% of iCCA harbor alterations amenable to precision oncology approaches, including fibroblast growth factor receptor 2 (FGFR2) fusions, isocitrate dehydrogenase 1 (IDH1) mutations, ERBB2 alterations, and BRAF mutations. In this review, we explore how this framework has reshaped liver cancer care and discuss the resulting breakthroughs in management and emerging directions that may further improve therapeutic strategies.
参考文献:
- 1. Hanahan D. Hallmarks of cancer-Then and now, and beyond. Cell. 2026;189(8):2254-2277. doi:10.1016/j.cell.2025.12.049
- 2. Yap TA, Manning HC, Sapra P, Mills GB, O'Connor MJ. Targeting genomic instability in cancer. Cell. 2026;189(8):2278-2306. doi:10.1016/j.cell.2026.03.035
- 3. Wong IT, Bailey C, Wu S, et al. A recipe for chaos: Extrachromosomal DNA and the hallmarks of cancer. Cell. 2026;189(8):2307-2321. doi:10.1016/j.cell.2026.03.011
- 4. Conrad M, Strasser A, Jost PJ, et al. Cell death in cancer. Cell. 2026;189(8):2322-2356. doi:10.1016/j.cell.2026.03.024
- 5. Hinterleitner C, Goldberg HV, McHugh D, Barthet VJA, Filliol A, Lowe SW. Senescence in cancer: Hallmarks, paradoxes, and therapeutic promise. Cell. 2026;189(8):2357-2378. doi:10.1016/j.cell.2026.03.005
- 6. Subudhi S, Lee S, Jain RK. Targeting angiogenesis: Lessons from 25 years of normalizing tumor vasculature. Cell. 2026;189(8):2379-2415. doi:10.1016/j.cell.2026.03.016
- 7. Marine JC, Bartok O, Sagie S, et al. Mapping intratumor heterogeneity across layers for advancing immunotherapy. Cell. 2026;189(8):2416-2440.doi:10.1016/j.cell.2026.03.025
- 8. Quail DF, Joyce JA. Cancer ecosystems: A dynamic interplay across scales. Cell. 2026;189(8):2441-2463. doi:10.1016/j.cell.2026.03.003
- 9. Winkler F, Heuer S, Althammer F, et al. Cancer neuroscience: The past, the present, and the road ahead. Cell. 2026;189(8):2464-2489. doi:10.1016/j.cell.2026.03.018
- 10. Llovet JM, Pinyol R, Affo S, et al. Hallmarks of liver cancer: Therapeutic implications. Cell. 2026;189(8):2490-2514. doi:10.1016/j.cell.2026.03.001